Release Of Information Template Mental Health
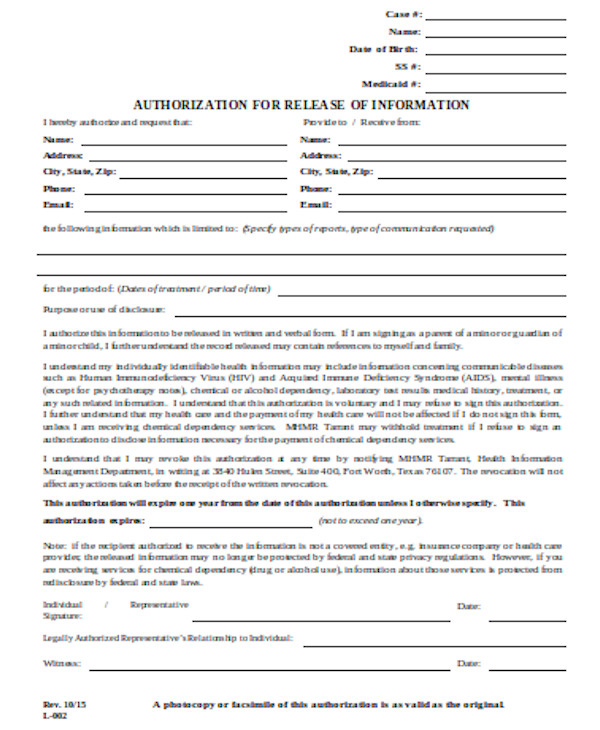
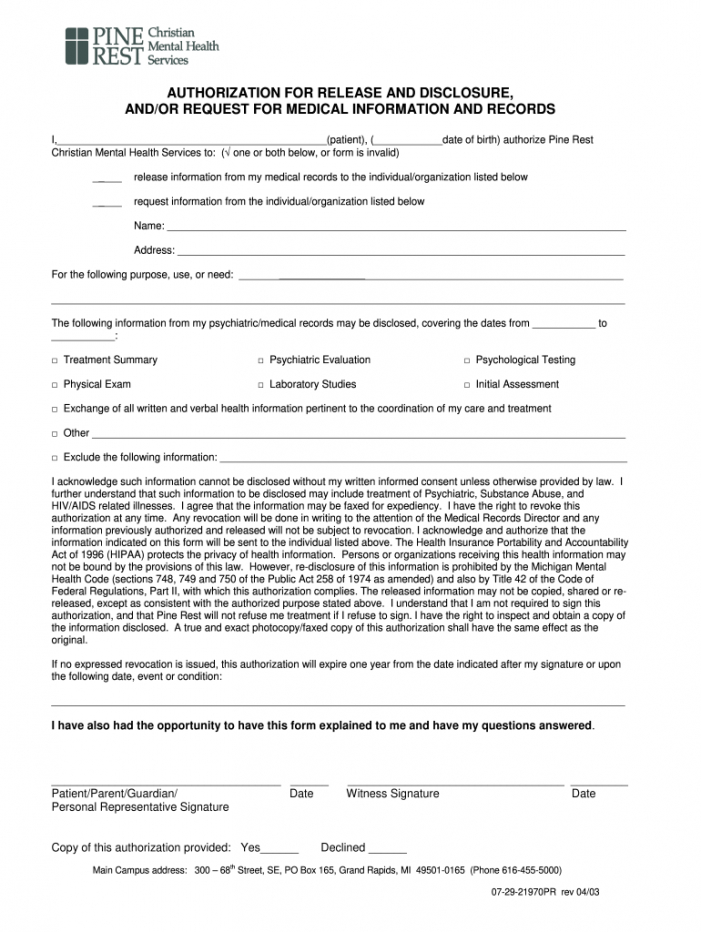
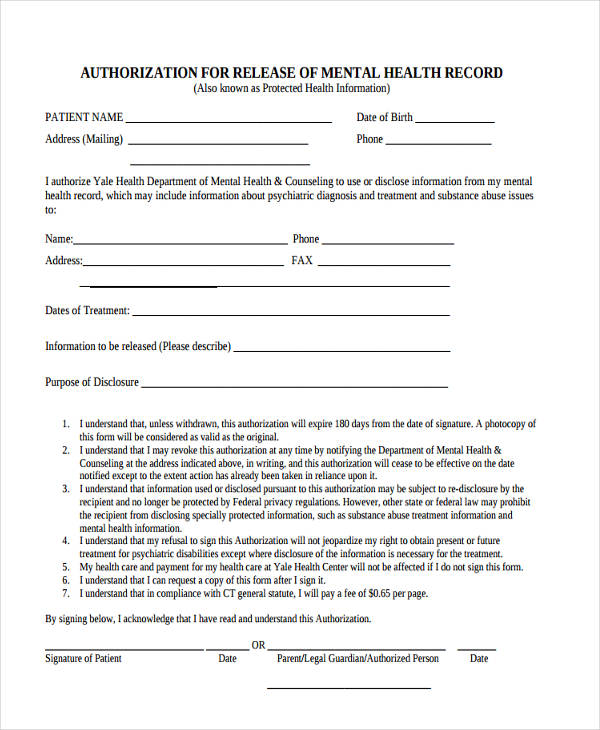
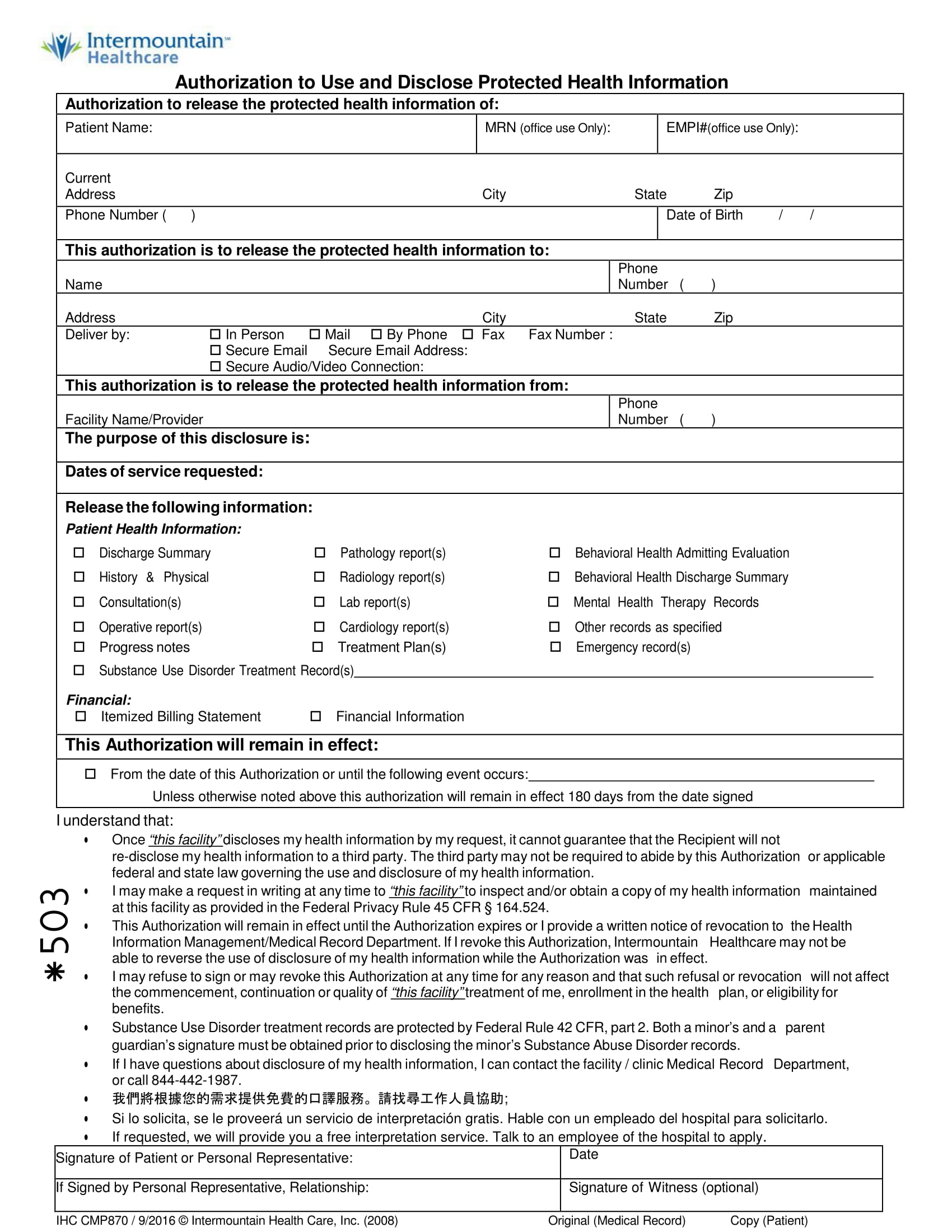
Release Of Information Template Mental Health - I authorize the named entity above (page 1) to use or disclose my health information in the manner described above. Our mental health release of information form was designed with your patient in mind. If you are unable to find the information you need, you can request records from your patient online services account or you may contact mayo. Sign it in a few. The person, company or agency named below:. Web authorization for release of mental health record (also known as protected health information) patient name. Edit your release of information form mental health online type text, add images, blackout confidential details, add comments, highlights and more. Web to release to name of agency/person/organization address (street,city, state and zip code) the information specified on page 2 of this form with the knowledge that such. The specific uses and limitations of the types of. Web • medical and mental health records are protected by federal and state confidentiality laws and regulations and cannot be released without my written consent unless otherwise. Web mental health treatment i, _____[insert name of patient/client], whose date of birth is _____, authorize [insert name of social work organization] to disclose to and/or obtain. Web zip am requesting this disclosure of information and records for the following purpose: Sign it in a few. At the request of the individual other: Web printable pdf includes license for 1. Easily customize your information release. Web mental health treatment i, _____[insert name of patient/client], whose date of birth is _____, authorize [insert name of social work organization] to disclose to and/or obtain. For the rest of your necessary intake forms, check out our easy intake packet, which includes the 7. Sign it in a few. Web authorize the release of. The specific uses and limitations of the types of. Web about the use or disclosure of my health information. These steps will empower your patient to take control of their mental. Web authorization for release of mental health record (also known as protected health information) patient name. Web printable pdf includes license for 1 person's unlimited use guaranteed safe checkout. Web authorization for the release of information is not sufficient for this purpose for client records applicable under federal law 42 cfr part 2. Web about the use or disclosure of my health information. Provide information to or request information from. Our mental health release of information form was designed with your patient in mind. I authorize the named entity. Web authorize greater nashua mental health center to: Web the rule is carefully balanced to allow uses and disclosures of information—including mental health information—for treatment and certain other. Sign it in a few. Web to release to name of agency/person/organization address (street,city, state and zip code) the information specified on page 2 of this form with the knowledge that such.. The person, company or agency named below:. Web mental health treatment i, _____[insert name of patient/client], whose date of birth is _____, authorize [insert name of social work organization] to disclose to and/or obtain. Web the rule is carefully balanced to allow uses and disclosures of information—including mental health information—for treatment and certain other. Web authorization for release of mental. Web about the use or disclosure of my health information. At the request of the individual other: Provide information to or request information from. Web to release to name of agency/person/organization address (street,city, state and zip code) the information specified on page 2 of this form with the knowledge that such. Our mental health release of information form was designed. If you are unable to find the information you need, you can request records from your patient online services account or you may contact mayo. As such, they have the option to specify what information is disclosed, how long the authorization will be valid for, and the purpose for the disclosure. I authorize the named entity above (page 1) to. Web authorize greater nashua mental health center to: Our mental health release of information form was designed with your patient in mind. Purpose or need for information: If you are unable to find the information you need, you can request records from your patient online services account or you may contact mayo. Ad answer simple questions to make an information. Web zip am requesting this disclosure of information and records for the following purpose: Purpose or need for information: Web mental health treatment i, _____[insert name of patient/client], whose date of birth is _____, authorize [insert name of social work organization] to disclose to and/or obtain. The specific uses and limitations of the types of. Our mental health release of. Web • medical and mental health records are protected by federal and state confidentiality laws and regulations and cannot be released without my written consent unless otherwise. Web printable pdf includes license for 1 person's unlimited use guaranteed safe checkout description reviews (1) q & a description this mental health release of. Web the rule is carefully balanced to allow uses and disclosures of information—including mental health information—for treatment and certain other. Easily customize your information release. The specific uses and limitations of the types of. This template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where. Web authorize greater nashua mental health center to: Provide information to or request information from. Web authorization for the release of information is not sufficient for this purpose for client records applicable under federal law 42 cfr part 2. This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family member or friend) such as an. Web zip am requesting this disclosure of information and records for the following purpose: Ad answer simple questions to make an information release on any device in minutes. Web authorization for release of mental health record (also known as protected health information) patient name. Web release of information form. At the request of the individual other: If you are unable to find the information you need, you can request records from your patient online services account or you may contact mayo. For the rest of your necessary intake forms, check out our easy intake packet, which includes the 7. I authorize the named entity above (page 1) to use or disclose my health information in the manner described above. Edit your release of information form mental health online type text, add images, blackout confidential details, add comments, highlights and more. Authorization to release information description of information to be used/disclosed: This template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where. Easily customize your information release. Sign it in a few. I understand that the information to be disclosed may include information about medical, psychiatric, drug and/or alcohol, mental health, social, and/or communicable. For the rest of your necessary intake forms, check out our easy intake packet, which includes the 7. At the request of the individual other: I authorize the named entity above (page 1) to use or disclose my health information in the manner described above. Our mental health release of information form was designed with your patient in mind. Web authorization for release of mental health record (also known as protected health information) patient name. Web authorize the release of any and all of the following medical, mental health and/or substance use disorder information, as specified, which may be contained in my. Web to release to name of agency/person/organization address (street,city, state and zip code) the information specified on page 2 of this form with the knowledge that such. This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family member or friend) such as an. Ad answer simple questions to make an information release on any device in minutes. If you are unable to find the information you need, you can request records from your patient online services account or you may contact mayo. The person, company or agency named below:. As such, they have the option to specify what information is disclosed, how long the authorization will be valid for, and the purpose for the disclosure.
Hospital Release form Template Lovely 9 Best Of Free Printable Hospital

FREE 13+ Sample Release of Information Forms in PDF MS Word
FREE 13+ Sample Release of Information Forms in PDF MS Word
Printable Release Of Information Form Pdf Fill Out And Sign Printable
FREE 17+ General Release of Information Forms in PDF Ms Word
FREE 13+ Health Information Forms in MS Word PDF

FREE 9+ Sample Release of Information Forms in MS Word PDF
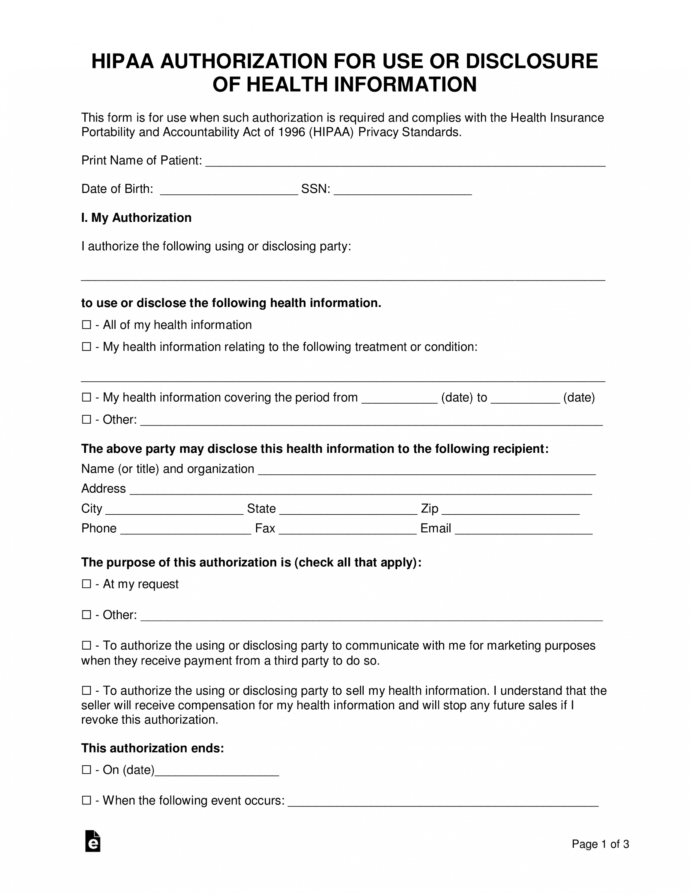
Free Free Medical Records Release Authorization Form Hipaa Mental

Counseling release of information template Fill out & sign online DocHub
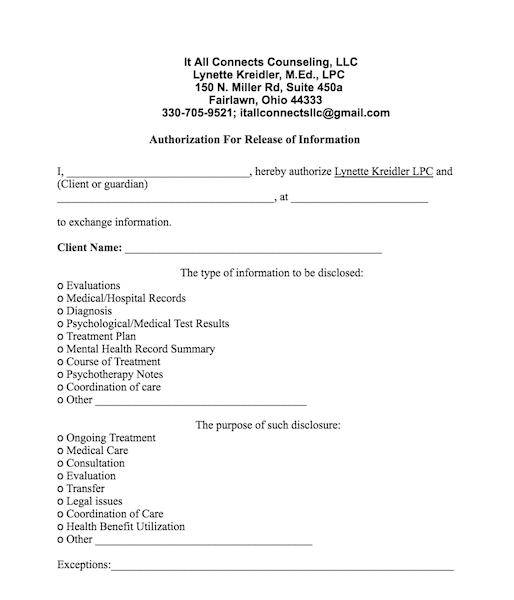
Forms — It All Connects Counseling — Fairlawn OH
Web Authorize Greater Nashua Mental Health Center To:
Web • Medical And Mental Health Records Are Protected By Federal And State Confidentiality Laws And Regulations And Cannot Be Released Without My Written Consent Unless Otherwise.
Edit Your Release Of Information Form Mental Health Online Type Text, Add Images, Blackout Confidential Details, Add Comments, Highlights And More.
The Specific Uses And Limitations Of The Types Of.
Related Post: