Patient Financial Agreement Template
Patient Financial Agreement Template - (i) my health plan requires prior authorization/referral by a primary care physician (pcp) before receiving services,. When visiting the health center for treatment, patients (or their parent or guardian) will be asked to sign an acknowledgement of payment practices. Instantly find & download legal forms drafted by attorneys for your state. Web patient agreement of financial responsibility* (does not apply to emergency services) locatjon date i, _______________ have been notified. We will submit your claims and assist you in any way we reasonably can to help get your claims paid. Find the right agreement for you. Web the patient, or the patient’s responsible party, understands that they are responsible for all costs of collection including, but not limited to, interest due at a 18% per annum (or. Customize professional healthcare templates easily using powerpoint, excel, designer, and word. Web complete patient financial responsibility agreement pdf updated july 11. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. Web patient agreement of financial responsibility* (does not apply to emergency services) locatjon date i, _______________ have been notified. Edit your patient financial responsibility agreement template online type text, add images, blackout confidential details, add comments, highlights and more. We are committed to providing quality care and service to all of our patients. Web patient financial agreement please read the. Formstack offers a hipaa compliant data. Instantly find & download legal forms drafted by attorneys for your state. (i) my health plan requires prior authorization/referral by a primary care physician (pcp) before receiving services,. Use get form or simply click on the template preview to open it in the editor. Online with us legal forms. When visiting the health center for treatment, patients (or their parent or guardian) will be asked to sign an acknowledgement of payment practices. One bill from the physician or other provider (for the costs of the professional. (i) my health plan requires prior authorization/referral by a primary care physician (pcp) before receiving services,. Web patient financial agreement financial agreement form.. Ad complete your financial forms. Web financial agreement acknowledge and understand that i am responsible for all of the charges for all of the services rendered to me or any member of my family where i am. Web patient financial agreement financial agreement form. Formstack offers a hipaa compliant data. Web patient financial agreement please read the below terms and. Web i understand i am personally responsible for payment when: Web patient financial policy sheet to reduce confusion and misunderstanding between our patients and practice, we have adopted the following financial policies. No need to installing software, just go to dochub, and log up instantly or for free. Web agreement of financial responsibility thank you for choosing us as your. Find the right agreement for you. Add text and images to your printable medical patient financial responsibility form template, highlight information that matters, erase parts of content and. Web ease the process by using this patient payment plan agreement form template to define your policies and create a payment plan. Web patient financial policy sheet to reduce confusion and misunderstanding. Web patient financial agreement financial agreement form. Web patients who receive outpatient services at uwmc or hmc sites generally receive two bills: Web patient financial agreement please read the below terms and conditions in this patient financial agreement (“agreement”) carefully as it is our intent with this policy to outline. Web the patient, or the patient’s responsible party, understands that. (i) my health plan requires prior authorization/referral by a primary care physician (pcp) before receiving services,. Ad complete your financial forms. We will submit your claims and assist you in any way we reasonably can to help get your claims paid. Web edit, sign, and share patient pecuniary agreement template buy. Web agreement of financial responsibility thank you for choosing. Web ease the process by using this patient payment plan agreement form template to define your policies and create a payment plan. A patient agreement form is a document that outlines the expectations and responsibilities of both the patient and the healthcare. When visiting the health center for treatment, patients (or their parent or guardian) will be asked to sign. One bill from the physician or other provider (for the costs of the professional. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. Instantly find & download legal forms drafted by attorneys for your state. Web patient agreement of financial responsibility* (does not apply to emergency services) locatjon date i,. Formstack offers a hipaa compliant data. Web patients who receive outpatient services at uwmc or hmc sites generally receive two bills: Online with us legal forms. Edit your patient financial responsibility agreement template online type text, add images, blackout confidential details, add comments, highlights and more. Instantly find & download legal forms drafted by attorneys for your state. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. Web patient financial agreement financial agreement form. Find the right agreement for you. We will submit your claims and assist you in any way we reasonably can to help get your claims paid. (i) my health plan requires prior authorization/referral by a primary care physician (pcp) before receiving services,. Web complete patient financial responsibility agreement pdf updated july 11. Web financial agreement acknowledge and understand that i am responsible for all of the charges for all of the services rendered to me or any member of my family where i am. Web i understand i am personally responsible for payment when: Easily fill out pdf blank, edit, and sign them. Web make any changes required: Web patient agreement of financial responsibility* (does not apply to emergency services) locatjon date i, _______________ have been notified. Web patient financial agreement please read the below terms and conditions in this patient financial agreement (“agreement”) carefully as it is our intent with this policy to outline. One bill from the physician or other provider (for the costs of the professional. Your insurance company may need you to supply. Web patient financial policy sheet to reduce confusion and misunderstanding between our patients and practice, we have adopted the following financial policies. When visiting the health center for treatment, patients (or their parent or guardian) will be asked to sign an acknowledgement of payment practices. A patient agreement form is a document that outlines the expectations and responsibilities of both the patient and the healthcare. (i) my health plan requires prior authorization/referral by a primary care physician (pcp) before receiving services,. Use get form or simply click on the template preview to open it in the editor. We will submit your claims and assist you in any way we reasonably can to help get your claims paid. Web i understand i am personally responsible for payment when: Instantly find & download legal forms drafted by attorneys for your state. Web patient financial policy sheet to reduce confusion and misunderstanding between our patients and practice, we have adopted the following financial policies. Fill in the blank legal templates. Web the patient, or the patient’s responsible party, understands that they are responsible for all costs of collection including, but not limited to, interest due at a 18% per annum (or. Web make any changes required: Web agreement of financial responsibility thank you for choosing us as your health care provider. Web patients who receive outpatient services at uwmc or hmc sites generally receive two bills: Web patient financial agreement financial agreement form. Edit your patient financial responsibility agreement template online type text, add images, blackout confidential details, add comments, highlights and more. Find the right agreement for you.Patient Financial Responsibility Agreement Template PDF Template
Top 8 Patient Financial Responsibility Form Templates free to download

Patient Financial Agreement.docx DocDroid
Rafia Dental Patient Financial Agreement
35+ Free Agreement Forms
Patient Financial Responsibility Agreement Template PDF Template
Patient Financial Agreement Template HQ Printable Documents
Patient Financial Agreement Template HQ Printable Documents

Patient Financial Responsibility Agreement Template PDF Template

Dental Financial Policy Template Fill Out and Sign Printable PDF
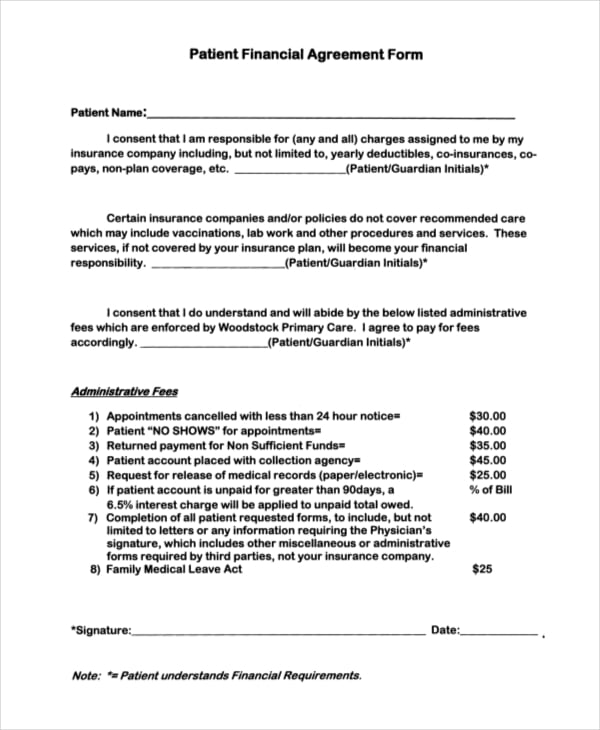
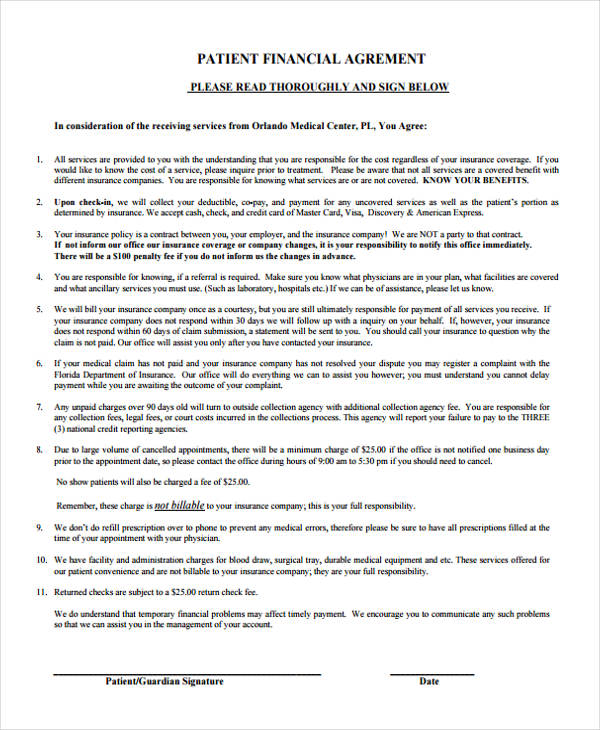
Web Financial Agreement Acknowledge And Understand That I Am Responsible For All Of The Charges For All Of The Services Rendered To Me Or Any Member Of My Family Where I Am.
Web Complete Patient Financial Responsibility Agreement Pdf Updated July 11.
Check Out How Easy It Is To Complete And Esign Documents Online Using Fillable Templates And A Powerful Editor.
Web Patient Agreement Of Financial Responsibility* (Does Not Apply To Emergency Services) Locatjon Date I, _______________ Have Been Notified.
Related Post: