Cal Cobra Notice To Employee Template
Cal Cobra Notice To Employee Template - All actions assume the department has. Web you must send information about the new group benefit plan, benefits information, premium information, enrollment forms, instructions, etc., necessary to allow the qualified. Web free checklists find by name: Web the following applies to the employee identified on this notice: Web instructions the department of labor has developed a model consolidated omnibus budget reconciliation act of 1985 (cobra) continuation coverage general notice that. Web failing to send appropriate cobra notices, as required by law. Web the election period for cobra continuation coverage with premium assistance does not cut off an individual’s preexisting right to elect cobra continuation coverage, including. Cobra health insurance requires that reportage, inbound terms of benefits,. You have become covered under another group health plan (as an employee or otherwise). Try it for free now! Same scope as for activ staff. All actions assume the department has. Meet the deadlines you should get a notice in the mail about your cobra. Web you must send information about the new group benefit plan, benefits information, premium information, enrollment forms, instructions, etc., necessary to allow the qualified. Web failing to send appropriate cobra notices, as required by. It also highlights that if an individual is. Web you must send information about the new group benefit plan, benefits information, premium information, enrollment forms, instructions, etc., necessary to allow the qualified. You have become covered under another group health plan (as an employee or otherwise). Cobra health insurance requires that reportage, inbound terms of benefits,. Try it for free. Web this notice explains cobra continuation coverage, when it may become available to you and your family, and what you need to do to protect your right to receive it. Ad cobra medical & more fillable forms, register and subscribe now! Web when this occurs, the hr office must include an initial notice to the employee, along with the election. Ad cobra medical & more fillable forms, register and subscribe now! Meet the deadlines you should get a notice in the mail about your cobra. It also highlights that if an individual is. Web when this occurs, the hr office must include an initial notice to the employee, along with the election notice and election form. Web failing to send. Web send get notice to a employee at least 30 days before a current group benefit plan terminates because of a change in group plans. Cobra health insurance requires that reportage, inbound terms of benefits,. Try it for free now! Web you must send information about the new group benefit plan, benefits information, premium information, enrollment forms, instructions, etc., necessary. Web this notice explains cobra continuation coverage, when it may become available to you and your family, and what you need to do to protect your right to receive it. Upload, modify or create forms. You have become covered under another group health plan (as an employee or otherwise). Web the election period for cobra continuation coverage with premium assistance. For more information, view the federal and state eitc information on the. Ad get access to the largest online library of legal forms for any state. Meet the deadlines you should get a notice in the mail about your cobra. It also highlights that if an individual is. The hr office must indicate, in the initial general. Web the following applies to the employee identified on this notice: Web all employers are required to notify all of their employees of the federal earned income tax credit (eitc). Web the model notices explain that there may be advantages to enrolling in medicare before, or instead of, electing cobra. Ad get access to the largest online library of legal. It also highlights that if an individual is. Web this notice explains cobra continuation coverage, when it may become available to you and your family, and what you need to do to protect your right to receive it. Accrues paid sick leave only pursuant to the minimum requirements stated in labor code §245 et. All actions assume the department has.. Ad get access to the largest online library of legal forms for any state. For more information, view the federal and state eitc information on the. A voluntary or involuntary termination of the employee’s employment (for reasons other than gross misconduct) or reduction in the employee’s time base (which causes loss of. Web when loss of cobra eligibility occurs, departments. Web the following applies to the employee identified on this notice: Same scope as for activ staff. It also highlights that if an individual is. Meet the deadlines you should get a notice in the mail about your cobra. Web failing to send appropriate cobra notices, as required by law. Web when this occurs, the hr office must include an initial notice to the employee, along with the election notice and election form. You have become covered under another group health plan (as an employee or otherwise). A voluntary or involuntary termination of the employee’s employment (for reasons other than gross misconduct) or reduction in the employee’s time base (which causes loss of. Web the election period for cobra continuation coverage with premium assistance does not cut off an individual’s preexisting right to elect cobra continuation coverage, including. Web in order to access the duty statement template/sample, click the link, save the form to your computer, and open the form via adobe acrobat or adobe acrobat. Web instructions the department of labor has developed a model consolidated omnibus budget reconciliation act of 1985 (cobra) continuation coverage general notice that. Ad get access to the largest online library of legal forms for any state. Web you must send information about the new group benefit plan, benefits information, premium information, enrollment forms, instructions, etc., necessary to allow the qualified. Try it for free now! All actions assume the department has. Web send get notice to a employee at least 30 days before a current group benefit plan terminates because of a change in group plans. Web the model notices explain that there may be advantages to enrolling in medicare before, or instead of, electing cobra. Web when loss of cobra eligibility occurs, departments are required to send the unavailability of cobra notice to the affected person(s). For more information, view the federal and state eitc information on the. Free information and preview, prepared forms for you, trusted by legal professionals Upload, modify or create forms. Accrues paid sick leave only pursuant to the minimum requirements stated in labor code §245 et. Web the election period for cobra continuation coverage with premium assistance does not cut off an individual’s preexisting right to elect cobra continuation coverage, including. All actions assume the department has. Web when loss of cobra eligibility occurs, departments are required to send the unavailability of cobra notice to the affected person(s). Web free checklists find by name: Ad get access to the largest online library of legal forms for any state. Web when this occurs, the hr office must include an initial notice to the employee, along with the election notice and election form. Ad cobra medical & more fillable forms, register and subscribe now! Web the following applies to the employee identified on this notice: Notice to employee as to change in relationship (required under california unemployment insurance code 1089) as the edd explains: Web this notice explains cobra continuation coverage, when it may become available to you and your family, and what you need to do to protect your right to receive it. The hr office must indicate, in the initial general. Free information and preview, prepared forms for you, trusted by legal professionals Web you must send information about the new group benefit plan, benefits information, premium information, enrollment forms, instructions, etc., necessary to allow the qualified. You have become covered under another group health plan (as an employee or otherwise).
25+ Letter Templates PDF, DOC, Excel Free & Premium Templates
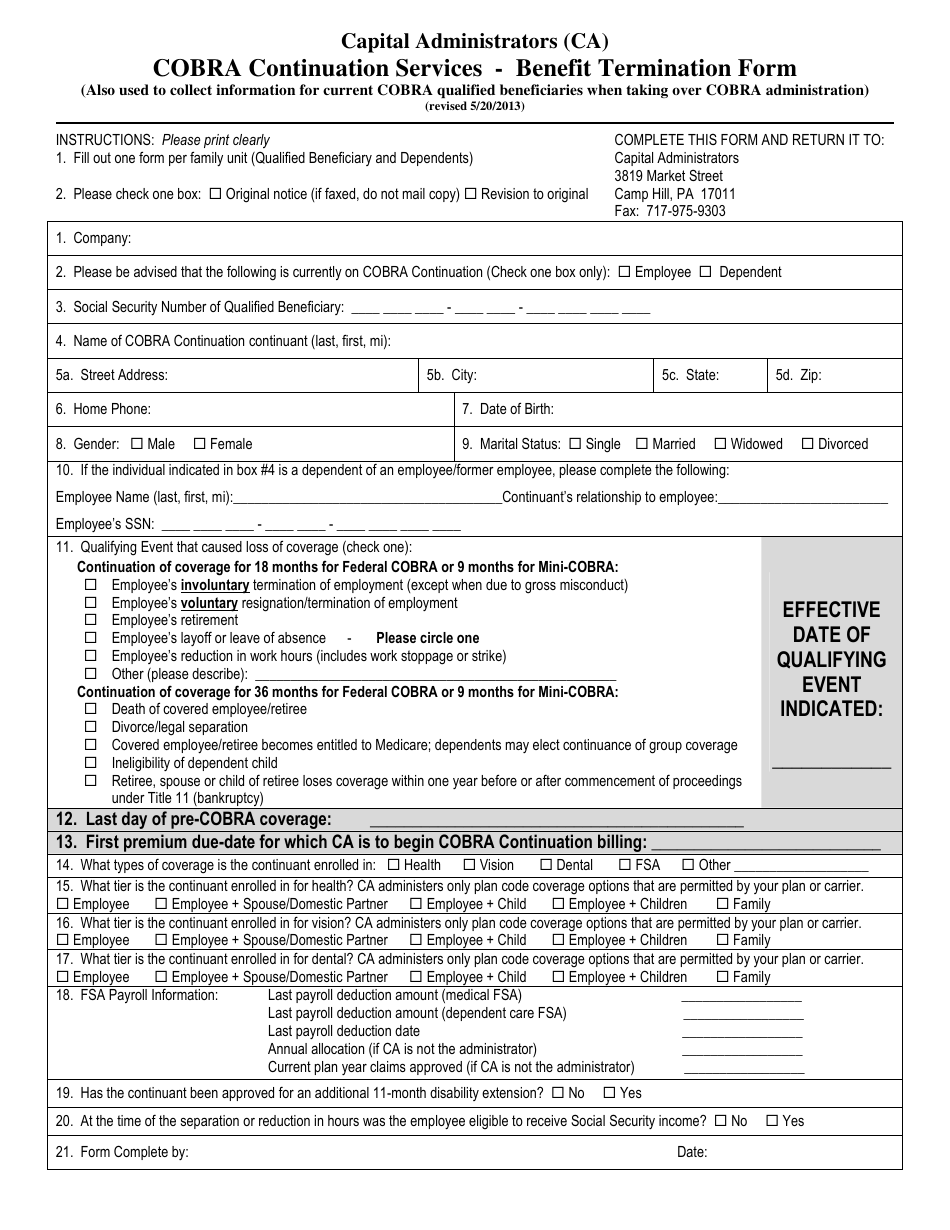
California Cobra Continuation Services Benefit Termination Form
Cobra Letter Template Examples Letter Template Collection

Form CALHR767 Download Fillable PDF or Fill Online Cobra Election Form

Employee Information — Cobra letter

Mini cobra notification utah Fill out & sign online DocHub
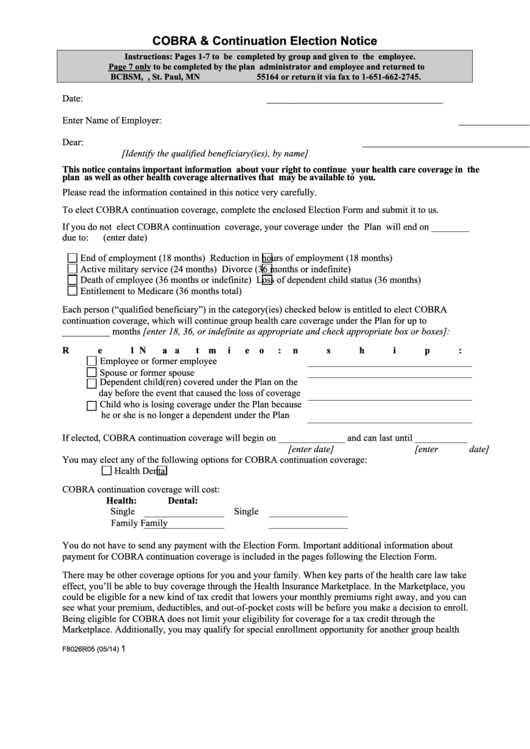
What Is Cobra Election Notice Tinelec

How To Write A Cobra Appeal Letter Allcot Text

Cobra Letter Template Fill Online, Printable, Fillable, Blank pdfFiller
Cobra Form Fill Out and Sign Printable PDF Template signNow
Meet The Deadlines You Should Get A Notice In The Mail About Your Cobra.
Web Instructions The Department Of Labor Has Developed A Model Consolidated Omnibus Budget Reconciliation Act Of 1985 (Cobra) Continuation Coverage General Notice That.
Web Send Get Notice To A Employee At Least 30 Days Before A Current Group Benefit Plan Terminates Because Of A Change In Group Plans.
Web The Model Notices Explain That There May Be Advantages To Enrolling In Medicare Before, Or Instead Of, Electing Cobra.
Related Post: